Drugs and surgeries marketed as 'gender affirming'
A new front in human liberation, or a medical scandal in the making?
Grainne Mhaol
9 January 2021
We fear that we have had front row seats to a medical scandal." (Comment from Psychologist in Britain to Sky News)(1)
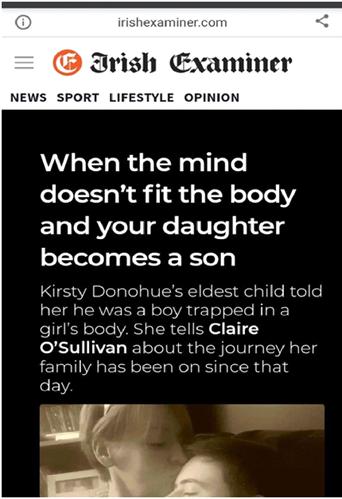
In the last two articles on this subject I spoke about sexism and homophobia driving gender identity ideology. (2) In the next few articles Im going to look at the concept and practice of what is called transitioning, or gender affirmation, which has both social and medical aspects. I'll be concentrating on the medical aspects in these articles.
Encouraging bodily alienation
The gender identity movement promotes bodily alienation. It does this by suggesting to children that their brain or personality sometimes doesnt match their physical sex, that they can be born in the wrong body(3), and that they can access medical interventions to fix their (healthy) body.
As Miranda Yardley, criticising this approach, has said: "There seems to me something uniquely cruel in telling children their bodies are wrong because they do not match the interests our culture deems appropriate for their sex."(4)
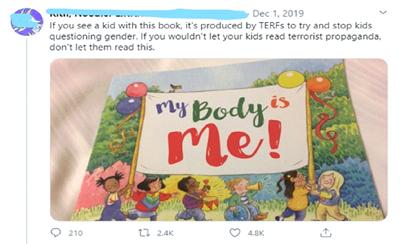
This is an example below of a book for children, which was written to encourage them to love the body they are in, being compared by a Transactivist to terrorist propaganda! (5)
Cosmetic Surgery promoted as the path to ones true self

The Gender Identity or Trans Right Movement promotes medications and cosmetic surgery as a way to become ones true self. It is important to remember that there is no biological medical reasons for these treatments. They are done to alter some bodily functions (e.g. stop women's periods) and to try to mimic the appearance of the opposite sex.
It says a lot about the condition of the Left that many left-identified activists are supporting what is essentially a massive sales-pitch for cosmetic treatments which is built on the promotion of body-image insecurity. Even experienced socialist politicians, such as Ruth Coppinger, who railed against Corportations...profiteeering through rainbow capitalism at Trans Pride in Dublin in 2018, supported the drive towards greater access to cosmetic treatments (that are potentially physically harmful), and the removal of what I would consider to be basic medical safeguarding, which she characterised as a doctor knows best attitude as to whether you can transition or get hormones or not(6). I'll be covering the problem with these drug treatments and surgeries in a later article, but it is worth pointing out there is no medical condition where a patient can self-diagnose and demand whatever treatments they want regardless of what the doctor thinks.
Interestingly, Dr. Aidan Kelly of GIDS [Gender Identity Development Service, based in Britain], who had been seeing Irish children with gender identity issues, seemed to almost grasp the regressive nature of transitioning children in a talk he gave in 2018:
the last thing we want is a young person changing their body to fit in with what they think societys rules are. There is a level of that in the society. We cant change society. Id love to be able to change society and take gender out of it all together, because then what does it matter, you just express and be what you want to be...? But theres a reality to some of society.(7) [my emphasis in bold]So if society didn't have sexist stereotypes there would be no need for us to transition anyone because they do not fit in with sexist stereotypes.
In a nutshell, medicaltransitioning is an alternative to changing society as a whole for the better, not the way to achieve a better society. We could do with a comeback of the Radical Psychiatry movement and the message it brought.
Interestingly, the famous critic of psychiatry, Thomas Szasz, recognised the anti-feminist core at the heart of Transexualism, or what we would now call gender identity ideology. In a book review published in The New York Times in 1979 he wrote: Miss Raymond has rightly seized on transsexualism as an emblem of modern society's unremitting though increasingly concealed antifeminism...The war between the sexes is a part of our, human heritage...If that war ever ends, it will be not because of a phony armistice arranged by doctors, but because men, women and children will place personal dignity before social sex-role identity. (8)
Transgender: Medical condition or identity?
There are a few seemingly contradictory strands in the gender identity movement. On the one hand you have a push for invasive medical treatments to become more readily available, and available to younger and younger children, but at the same time a push to de-medicalise the label of Transgender and have it be more of an identity, so that anyone can say they are Transgender without any diagnosis of gender dysphoria (a desire to be the opposite sex as well as an extreme discomfort with one's own sex), or desire to have any medical intervention. They also want people who openly state that they have no medical or psychiatric condition to be able to access certain surgeries and medications on the public health system, or via health insurance.
Whilst these strands seem contradictory on the surface, the over-riding principle is a hyper-individualism, where people are who they say they are, and a consumerist attitude towards medicine, where the customer should be able to get what they want.
A good example of how identitarianism and medical consumerism can co-exist can be seen in a documentary from Sweden on Transgenderism. A parent with a daughter who identifies as male was told by a clinic:
The answer we got was, We dont say no to anyone. We affirm everyone who comes to us, and its very important to affirm this, not to argue. Its a question of identity. Not a diagnosis, a question of identity.(9)A consultant from the Anova Clinic in Sweden, Cecilia Dhejne, shows that they adopt this sort of approach at the clinic when she says:
Its been many years since we didnt agree with the patient...When someone comes to talk to us we dont say no(9)A former patient, Johanna Berling, who attended the Anova clinc says this about her experience there: The only people I trusted to determine if I was trans, was the Anova clinic. And their first question was, When do you want to start on testosterone? (9)
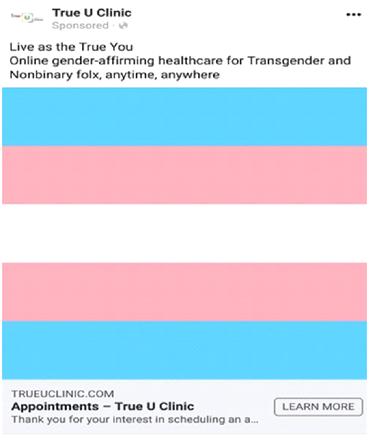
This image below is from
an advertisement for a clinic in the US. It shows cosmetic medical interventions
being promoted as the path to ones true self
Campaigning for the removal of psychiatric screening before medical interventions
The trajectory of the Trans-Rights-Movement internationally is to campaign for the removal of psychiatric/psychological screenings before medical interventions. The Irish campaigning group, This is me, seems to support going along this route. This is a recent comment from the main person running that group, Noah Halpin:
Countries like New Zealand, Australia, and Germany follow international best practice standards of care which allow people who are transgender to access treatments and surgery without undergoing mental health evaluation or referral from a mental health specialist. (10)The removal of screening, of course, potentially massively increases the market in this area, as well as increasing the risk of harm. The profit-motive is probably part of the reason this model is being implemented in some places.
The affirmation-only approach and the informed consent model
Sometimes the Trans-rights-movement argues that what it wants is the informed consent model for what is called Transgender healthcare. This sounds quite reasonable, but like so many other things in this movement the label is misleading.
Informed consent in medicine normally means that the doctor discusses the relevant treatment options with the patient, and points out the potential positive and negative outcomes. This is because many medicines or other treatments have potentially negative side-effects and it is important that the patient is properly informed so that they can decide whether or not they want to take the risk.
But some Trans-Right-Activists promote a model of Informed consent which is effectively treatment on demand. They think that once the doctor informs the patient of the risks, the doctor should prescribe the drugs the patient wants, or refer for surgery. They argue against the need for a psychiatric diagnosis or screening before accessing hormones or surgery. Some even think that a need for the doctor to be persuaded that the patient will benefit mentally or physically from medicines before prescribing them is overly burdensome.(11) This is a free market consumerist approach to medicine rather than one based on a rational health-orientated approach, or one with patient safety at its core.
Affirmation-only is similar in that it argues that the doctor should affirm the claims of the patient (effectively that the doctor should affirm a self-diagnosis by a patient, and normally agree to prescribe or refer for the treatments they want). Again this is dispensing with normal medical practice and opening up patients to great risks.
This is a recent tweet below from Transgender Equality Network Ireland promoting the affirmation-only approach.

Medical regulation a necessity to reduce harm
Frustrating as it might be sometimes, not all medical regulation or gate-keeping is bad. Without regulations, patients, or potential patients, can easily become prey to quacks and charlatans, especially if they are led to believe that some drug or intervention will alleviate their symptoms or distress. This is why we have things like drug trials and regulation of medicines, so that claims can be objectively evaluated (even with these safeguards there are still problems due to error, bias, and corruption).
In the same way, the doctor can't just accept a self-diagnosis at face-value. This would lead to misdiagnosis and harm to patients.
As one former patient astutely put it Healthcare professionals should be the impartial ones...The role of healthcare professionals is to diagnose, not to be nice(12)
Even though I think there is a fundamental problem with medical transitioning, having some psychiatric or medical screening acts as a barrier to a total free for all, and should reduce harms.
A few doctors, in a letter sent to the British Medical Journal, suggested a cautious approach, especially when dealing with children: While respecting individuals right to a different viewpoint, it is neither mandatory to affirm their beliefs nor automatic that transition is the goal, particularly when dealing with children, adolescents and young adults. These risk closing the open future, as well as life-long physical problems including lack of sexual function, infertility and medical dependency. With 85% amongst referred transgender children desistance [desistance means they will no longer identify as the opposite sex] and increasing awareness of detransitioning, unquestioning affirmation as a pathway that leads gender dysphoric patients to irreversible interventions cannot be considered sole or best practice."[my emphasis] (13)
Susie Green, CEO of the British-based Mermaids charity below arguing for access to surgery for minors, and the removal of psychiatric assessment before surgeries. Incidentally, contrary to what is said here, counselling and sometimes psychological assessment, is done before some non-transgender related testing and treatments.
Who loses from an affirmation-only approach?
If an affirmation only model is introduced it will disproportionally negatively impact Gay, lesbian and bisexual young people. Even therapists who have worked in the field have concerns that transitioning young people is a new form of Gay Conversion Therapy.(14)

Adopting an affirmation-only
approach would also disproportionately negatively affect autistic people,
and people who end up identifying as transgender, or the opposite sex,
or as belonging to neither sex, after trauma such as the death of a parent
or sexual abuse. They have a higher likelihood of being seen at gender
identity clinics for young people than the general population, and put
on a path of lifelong medicalisation and potential sterilisation.
In the next article I will
take a more in-depth look at who is being seen at the gender identity clinics
for young people, and why, if anything, this should lead us to adopt a
position of greater, and not lesser, caution when dealing with these patients.
References
(2) http://www.socialistdemocracy.org/RecentArticles/RecentSocialismFeminismTransgenderPoliticsPartOne.html
http://www.socialistdemocracy.org/RecentArticles/RecentGenderIdentityIdeologyTransRightsMovementHomophobia.html
(3) For examples in the media
see https://threadreaderapp.com/thread/1309648257681743873?refresh=1603580593
In this documentary
also the head teacher is mentioned as explaining what being transgender
is to the school assembly: she showed a diagram of what it means to be
in a boys body but have a girls brain (this is what professionals are
being taught by transgender groups on professional training courses). https://www.youtube.com/watch?v=0IYYH43O4oc&feature=youtu.be
(5) This was also reported by Pink News in this ridiculous way. https://www.pinknews.co.uk/2019/12/03/transgender-trend-children-book-anti-trans-terrorist-propaganda-my-body-is-me/
(6) https://www.youtube.com/watch?v=v8hSDeRagvQ
(7) Dr. Aidan Kelly is a clinical psychologist working at the Gender Identity Development Service at the Tavistock Centre in London. He was the lead for the services Dublin satellite clinic. https://www.youtube.com/watch?v=kPlCGBBcw90
(8) https://www.nytimes.com/1979/06/10/archives/male-and-female-created-he-them-transexual.html
(9) https://www.youtube.com/watch?v=sJGAoNbHYzk
(10) https://dublininquirer.com/2020/12/09/noah-transgender-healthcare-in-ireland-is-inadequate
See this piece also https://www.rte.ie/news/ireland/2019/0922/1077496-trans-healthcare/
(11) This is an example of this attitude:
So they see it as an unnecessary burden of proof that the doctor should be persuaded that the patient will benefit mentally or physically from the medication. Contrary to the impression they give, almost all other medical practice involves medical gate-keeping, and a presumption that the doctor prescribe medicine only if they think the patient will benefit from it. The only exception really is many cosmetic surgical treatments, which are done more on a demand basis, and are driven by the profit motive and not based on the needs of, or potential benefit to, the patient.
(12) Johanna Berling https://www.youtube.com/watch?v=73-mLwWIgwU
(13) Susan Bewley, Margaret McCartney, Lucy Griffin, Richard Byng https://www.bmj.com/content/364/bmj.l245
(14) https://www.thetimes.co.uk/article/it-feels-like-conversion-therapy-for-gay-children-say-clinicians-pvsckdvq2I
I also covered this issue
in this article: http://www.socialistdemocracy.org/RecentArticles/RecentGenderIdentityIdeologyTransRightsMovementHomophobia.html